Designing IT to make Healthcare Safer
1) Make you more aware of avoidable computer safety hazards in modern hospitals.
2) Encourage you to view the complete lecture Designing IT to make Healthcare Safer
- at Gresham College UK, Feb 2014
The ideas, pictures and text were grossly stolen from the presentation above.:
Professor Harold Thimbleby (quoting much from Massachusetts General Hospital) effectively presents his case that better equipment and software design (especially the user interface) will prevent much confusion and many/most hospital "human" errors.
The pictures presented here are about 1/4 of the images presented in the first half of his presentation -
This web page is a teaser to get you to see the "real thing" (above) :-)
| This is Professor Harold Thimbleby starting out on his presentation. |
| He starts by showing the great improvements in automotive safety. He shows a video of a test crash of a 1950s car against a modern car. The 1950s car would certainly killed the driver, while the driver of the modern car would be only bruised. This Ralph Nadar book helped start the revolution. |
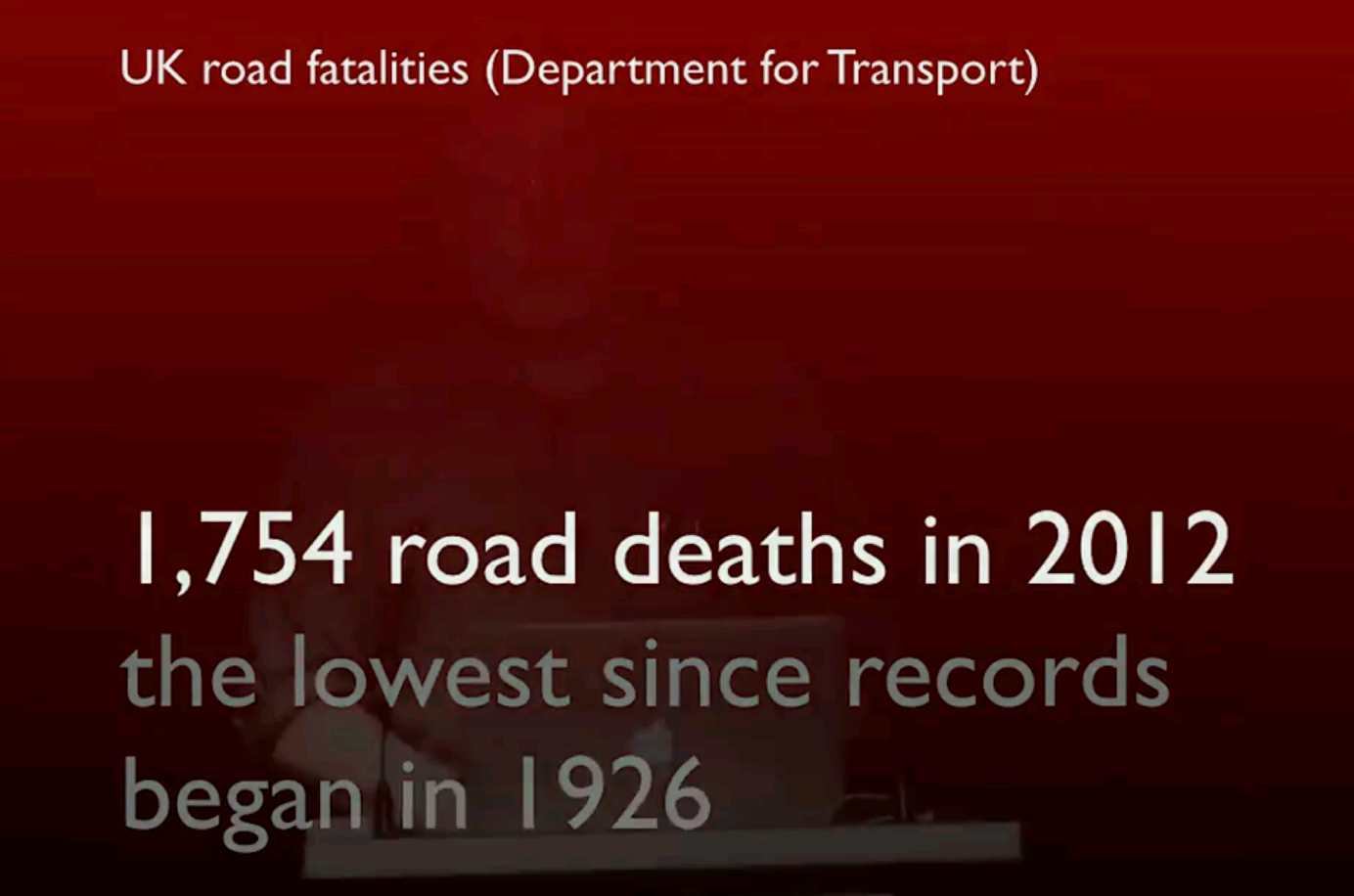
| Now he compares 1,754 UK road deaths per year vs |
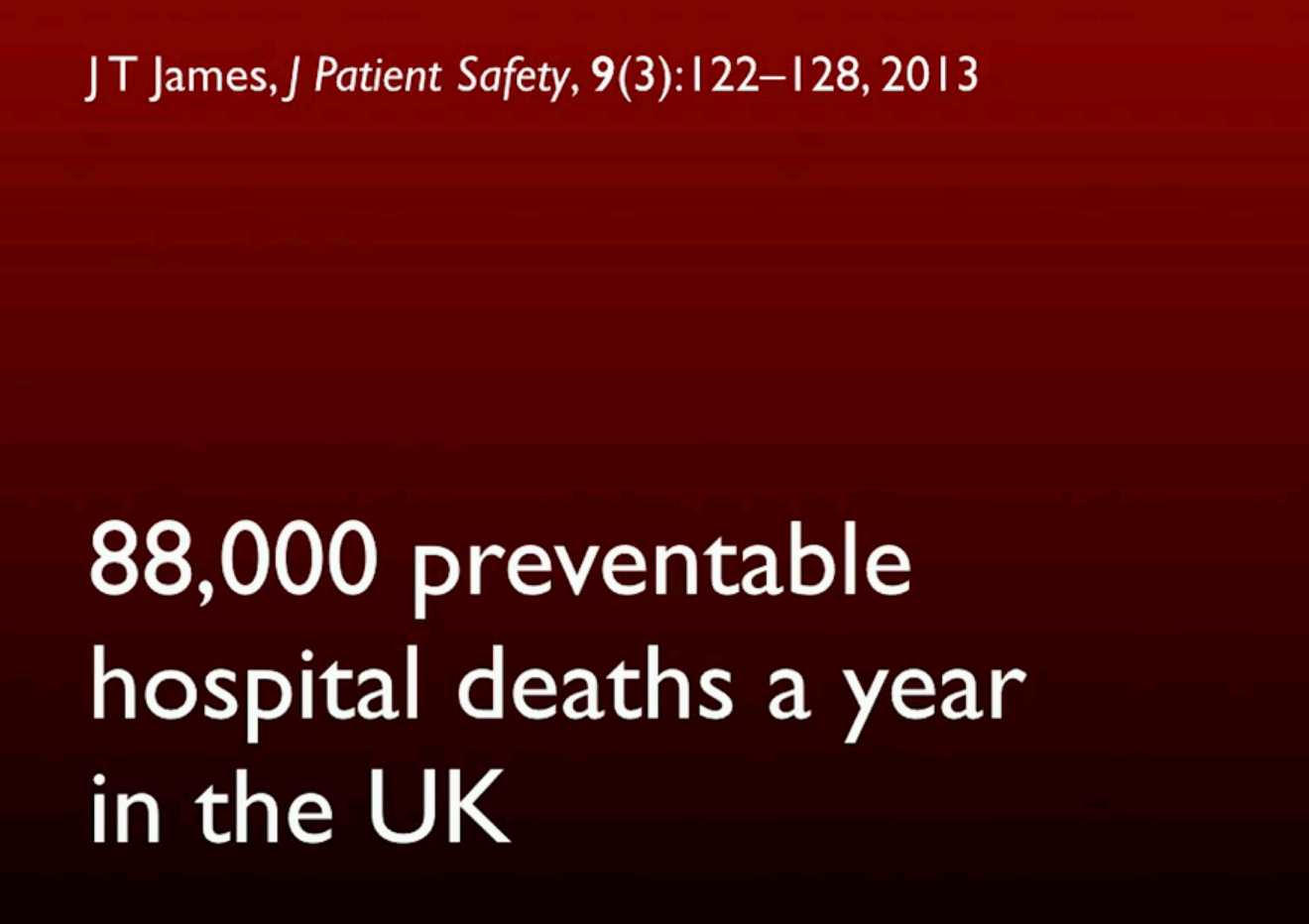
| an estimated (likely under-reported) 88,000 preventable hospital deaths per year. |
| Somewhat tongue-in-cheek - |
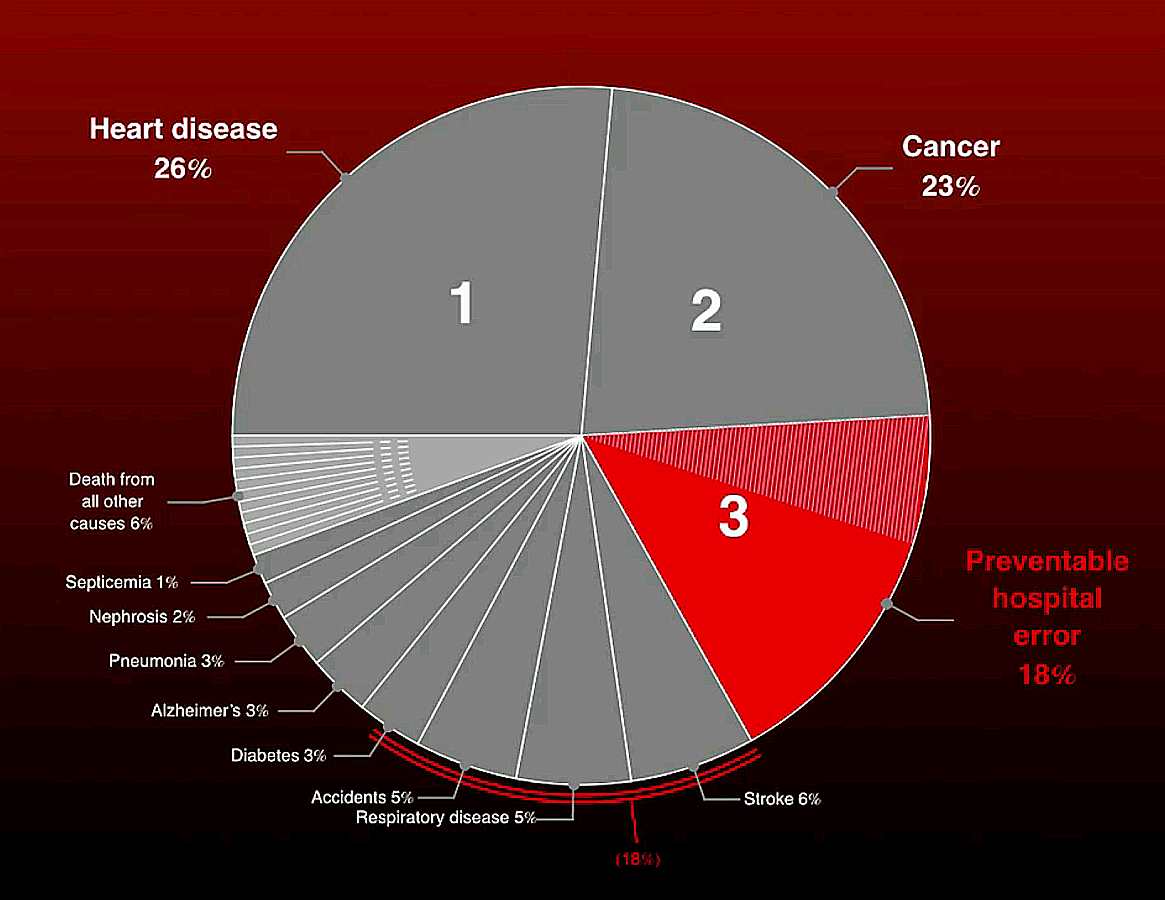
| 3rd Leading Cause of Death in the UK |
| A definite problem, detailed further on ... |

| Many many computers (embedded in other systems) in the hospital environment. (pink arrows) |
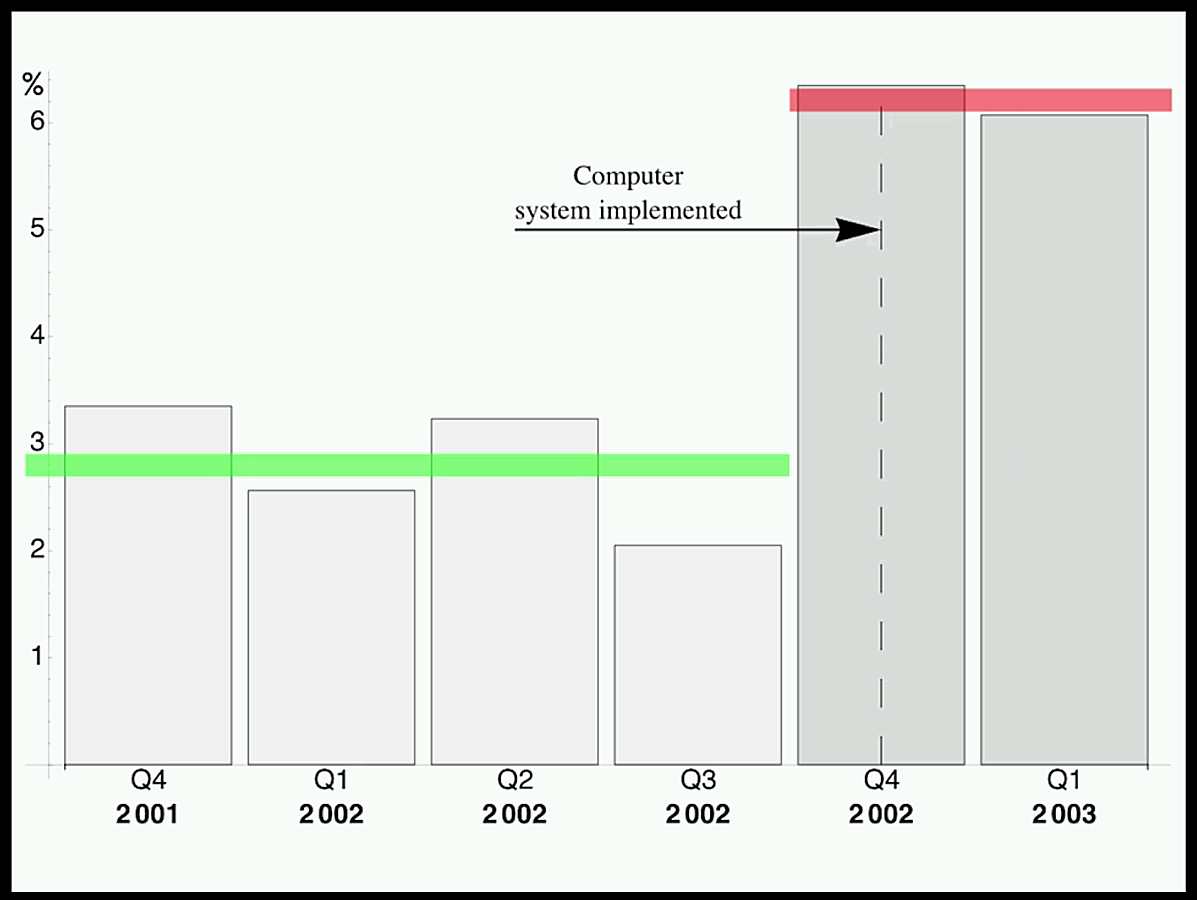
| Ward deaths before and after a computer system was installed -
The professor points out that every minute a nurse is on a keyboard is a minute lost in active patient care. |

| A sample of the current infusion pumps at Massachusetts General Hospital. Note the wild differences in keyboard layouts, multi-function keys, displays, ... He later point out that the two yellow "Body Guard" pumps have the same model numbers, but no other apparent similarities. Imagine the training problems, usage confusion of busy nurses ... |
We are about 1/4 of the way through the professor's presentation. He goes on with tragic examples of very easily made blunders.
Now we get into the actual errors -

| This infusion pump discards the decimal point if three digits have been input,
causing ten times the desired medication, unless the nurse is watching very carefully.
And more and more "human factors" blunders ... and deaths ... |
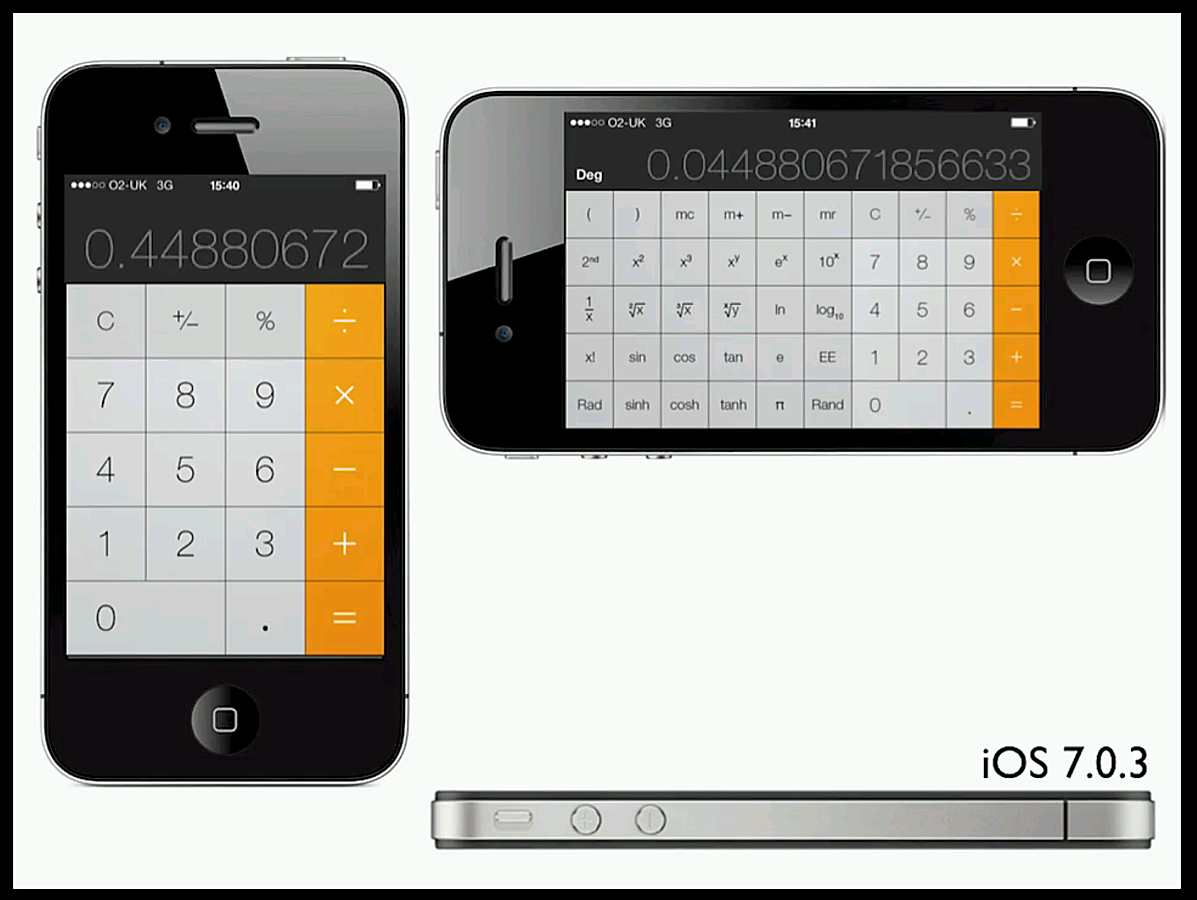
| And a Casio calculator that throws away digits that don't fit the display, giving errors of x10 or more.
Here is an iPhone with two different answers to the test problem, correct if horizontal where no digits were discarded, and off by x10 if the problem was entered when the machine was vertical. |
"Calculators should not be used in hospitals, because they are unsafe. They allow you to make slips, and they don't care."
We are now almost half way through the professor's presentation ...
I think you will be fascinated, and very concerned , if you watch the whole presentation
Designing IT to make Healthcare Safer
The last half shows how to develop better designed products, (user testing and feedback among others),
and how to get the better products into hospitals ...
And also there should be tests during the product life to assure correct performance and calibration.
Here is his web site, CHI-MED
[ My comment, any proper electronics lab periodically
has its equipment checked for function and calibration, with a sticker on it to show the fact and date.
Complex medical equipment apparently doesn't presently get this verification. ]
A note: The aircraft industry safety record has greatly improved over the years. There are vigorous investigations of "incidents" by outside technically competent organizations, and vigorous enforcement of the "recommendations". Also the pilot's unions have been vigorous in pointing out the why's of "pilot error", defending pilots and pointing the finger at poor design and procedures. Apparently the nurse's unions are more passive?
Date of web page May 31, 2017, by Ed Thelen ;-))